What
is Spinal Decompression?
By Thomas A. Gionis,
MD, JD, MBA, MHA, FICS, FRCS, and Eric Groteke, DC, CCIC
The outcome of
a clinical study evaluating the effect of nonsurgical intervention
on symptoms of spine patients with herniated and degenerative disc
disease is presented.
This
clinical outcomes study was performed to evaluate the effect of spinal
decompression on symptoms and physical findings of patients with herniated
and degenerative disc disease. Results showed that 86% of the 219
patients who completed the therapy reported immediate resolution of
symptoms, while 84% remained pain-free 90 days post-treatment. Physical
examination findings showed improvement in 92% of the 219 patients,
and remained intact in 89% of these patients 90 days after treatment.
This study shows that disc disease—the most common cause of back
pain, which costs the American health care system more than $50 billion
annually—can be cost-effectively treated using spinal decompression.
The cost for successful non-surgical therapy is less than a tenth
of that for surgery. These results show that biotechnological advances
of spinal decompression reveal promising results for the future of
effective management of patients with disc herniation and degenerative
disc diseases. Long-term outcome studies are needed to determine if
non-surgical treatment prevents later surgery, or merely delays it.
INTRODUCTION:
ADVANCES IN BIOTECHNOLOGY
With the recent
advances in biotechnology, spinal decompression has evolved into a
cost-effective nonsurgical treatment for herniated and degenerative
spinal disc disease, one of the major causes of back pain. This nonsurgical
treatment for herniated and degenerative spinal disc disease works
on the affected spinal segment by significantly reducing intradiscal
pressures.1 Chronic low back pain disability is the most expensive
benign condition that is medically treated in industrial countries.
It is also the number one cause of disability in persons under age
45. After 45, it is the third leading cause of disability.2 Disc disease
costs the health care system more than $50 billion a year.
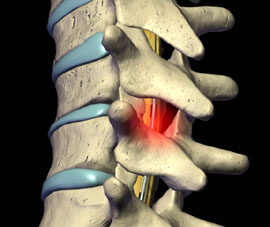
The intervertebral
disc is made up of sheets of fibers that form a fibrocartilaginous
structure, which encapsulates the inner mucopolysaccharide gel nucleus.
The outer wall and gel act hydrodynamically. The intrinsic pressure
of the fluid within the semirigid enclosed outer wall allows hydrodynamic
activity, making the intervertebral disc a mechanical structure.3
As a person utilizes various normal ranges of motion, spinal discs
deform as a result of pressure changes within the disc.4 The disc
deforms, causing nuclear migration and elongation of annular fibers.
Osteophytes develop along the junction of vertebral bodies and discs,
causing a disease known as spondylosis. This disc narrows from the
alteration of the nucleus pulposus, which changes from a gelatinous
consistency to a more fibrous nature as the aging process continues.
The disc space thins with sclerosis of the cartilaginous end plates
and new bone formation around the periphery of the contiguous vertebral
surfaces. The altered mechanics place stress on the posterior diarthrodial
joints, causing them to lose their normal nuclear fulcrum for movement.
With the loss of disc space, the plane of articulation of the facet
surface is no longer congruous. This stress results in degenerative
arthritis of the articular surfaces.
This is especially
important in occupational repetitive injuries, which make up a majority
of work-related injuries. When disc degeneration occurs, the layers
of the annulus can separate in places and form circumferential tears.
Several of these circumferential tears may unite and result in a radial
tear where the material may herniate to produce disc herniation or
prolapse. Even though a disc herniation may not occur, the annulus
produces weakening, circumferential bulging, and loss of intervertebral
disc height. As a result, discograms at this stage usually reveal
reduced interdiscal pressure.
The early changes
that have been identified in the nucleus pulposus and annulus fibrosis
are probably biomechanical and relate to aging. Any additional trauma
on these changes can speed up the process of degeneration. When there
is a discogenic injury, physical displacement occurs, as well as tissue
edema and muscle spasm, which increase the intradiscal pressures and
restrict fluid migration.6 Additionally, compression injuries causing
an endplate fracture can predispose the disc to degeneration in the
future.
The alteration
of normal kinetics is the most prevalent cause of lower back pain
and disc disruption and thus it is vital to maintain homeostasis in
and around the spinal disc; Yong-Hing and Kirkaldy-Willis7 have correlated
this degeneration to clinical symptoms. The three clinical stages
of spinal degeneration include:
Stage of Dysfunction.
There is little pathology and symptoms are subtle or absent. The diagnosis
of Lumbalgia and rotatory strain are commonly used.
Stage of Instability.
Abnormal movement of the motion segment of instability exists and
the patient complains of moderate symptoms with objective findings.
Conservative care is used and sometimes surgery is indicated.
Stage of Stabilization.
The third phase where there are severe degenerative changes of the
disc and facets reduce motion with likely stenosis.
Spinal decompression
has been shown to decompress the disc space, and in the clinical picture
of low back pain is distinguishable from conventional spinal traction.8,9
According to the literature, traditional traction has proven to be
less effective and biomechanically inadequate to produce optimal therapeutic
results.8-11 In fact, one study by Mangion et al concluded that any
benefit derived from continuous traction devices was due to enforced
immobilization rather than actual traction.10 In another study, Weber
compared patients treated with traction to a control group that had
simulated traction and demonstrated no significant differences.11
Research confirms that traditional traction does not produce spinal
decompression. Instead, decompression, that is, unloading due to distraction
and positioning of the intervertebral discs and facet joints of the
lumbar spine, has been proven an effective treatment for herniated
and degenerative disc disease, by producing and sustaining negative
intradiscal pressure in the disc space. In agreement with Nachemon’s
findings and Yong-Hing and Kirkaldy-Willis,1 spinal decompression
treatment for low back pain intervenes in the natural history of spinal
degeneration.7,12 Matthews13 used epidurography to study patients
thought to have lumbar disc protrusion. With applied forces of 120
pounds x 20 minutes, he was able to demonstrate that the contrast
material was drawn into the disc spaces by osmotic changes. Goldfish14
speculates that the degenerated disc may benefit by lowering intradiscal
pressure, affecting the nutritional state of the nucleus pulposus.
Ramos and Martin8 showed by precisely directed distraction forces,
intradiscal pressure could dramatically drop into a negative range.
A study by Onel et al15 reported the positive effects of distraction
on the disc with contour changes by computed tomography imaging. High
intradiscal pressures associated with both herniated and degenerated
discs interfere with the restoration of homeostasis and repair of
injured tissue.
Biotechnological
advances have fostered the design of Food and Drug Administration-approved
ergonomic devices that decompress the intervertebral discs. The biomechanics
of these decompression/reduction machines work by decompression at
the specific disc level that is diagnosed from finding on a comprehensive
physical examination and the appropriate diagnostic imaging studies.
The angle of decompression to the affected level causes a negative
pressure intradiscally that creates an osmotic pressure gradient for
nutrients, water, and blood to flow into the degenerated and/or herniated
disc thereby allowing the phases of healing to take place.
This clinical
outcomes study, which was performed to evaluate the effect of spinal
decompression on symptoms of patients with herniated and degenerative
disc disease, showed that 86% of the 219 patients who completed therapy
reported immediate resolution of symptoms, and 84% of those remained
pain-free 90 days post-treatment. Physical examination findings revealed
improvement in 92% of the 219 patients who completed the therapy.
METHODS
The study group
included 229 people, randomly chosen from 500 patients who had symptoms
associated with herniated and degenerative disc disease that had been
ongoing for at least 4 weeks. Inclusion criteria included pain due
to herniated and bulging lumbar discs that is more than 4 weeks old,
or persistent pain from degenerated discs not responding to 4 weeks
of conservative therapy. All patients had to be available for 4 weeks
of treatment protocol, be at least 18 years of age, and have an MRI
within 6 months. Those patients who had previous back surgery were
excluded. Of note, 73 of the patients had experienced one to three
epidural injections prior to this episode of back pain and 22 of those
patients had epidurals for their current condition. Measurements were
taken before the treatments began and again at week two, four, six,
and 90 days post treatment. At each testing point a questionnaire
and physical examination were performed without prior documentation
present in order to avoid bias. Testing included the Oswetry questionnaire,
which was utilized to quantify information related to measurement
of symptoms and functional status. Ten categories of questions about
everyday activities were asked prior to the first session and again
after treatment and 30 days following the last treatment.
Testing also consisted
of a modified physical examination, including evaluation of reflexes
(normal, sluggish, or absent), gait evaluation, the presence of kyphosis,
and a straight leg raising test (radiating pain into the lower back
and leg was categorized when raising the leg over 30 degrees or less
is considered positive, but if pain remained isolated in the lower
back, it was considered negative). Lumbar range of motion was measured
with an ergonometer. Limitations ranging from normal to over 15 degrees
in flexion and over 10 degrees in rotation and extension were positive
findings. The investigator used pinprick and soft touch to determine
the presence of gross sensory deficit in the lower extremities.
Of the 229 patients
selected, only 10 patients did not complete the treatment protocol.
Reasons for noncompletion included transportation issues, family emergencies,
scheduling conflicts, lack of motivation, and transient discomfort.
The patient protocol provided for 20 treatments of spinal decompression
over a 6-week course of therapy. Each session consisted of a 45-minute
treatment on the equipment followed by 15 minutes of ice and interferential
frequency therapy to consolidate the lumbar paravertebral muscles.
The patient regimen included 2 weeks of daily spinal decompression
treatment (5 days per week), followed by three sessions per week for
2 weeks, concluding with two sessions per week for the remaining 2
weeks of therapy
On the first day
of treatment, the applied pressure was measured as one half of the
person’s body weight minus 10 pounds, followed on the second
day with one half of the person’s body weight. The pressure placed
for the remainder of the 18 sessions was equivalent to one half of
the patient’s body weight plus an additional 10 pounds. The angle
of treatment was set according to manufacturer’s protocol after
identifying a specific lumbar disc correlated with MRI findings. A
session would begin with the patient being fitted with a customized
lower and upper harness to fit their specific body frame. The patient
would step onto a platform located at the base of the equipment, which
simultaneously calculated body weight and determined proper treatment
pressure. The patient was then lowered into the supine position, where
the investigator would align the split of table with the top of the
patient’s iliac crest. A pneumatic air pump was used to automatically
increase lordosis of the lumbar spine for patient comfort. The patient’s
chest harness was attached and tightened to the table. An automatic
shoulder support system tightened and affixed the patient’s upper
body. A knee pillow was placed to maintain slight flexion of the knees.
With use of the previously calculated treatment pressures, spinal
decompression was then applied. After treatment, the patient received
15 minutes of interferential frequency (80 to 120 Hz) therapy and
cold packs to consolidate paravertebral muscles.
During the initial
2 weeks of treatment, the patients were instructed to wear lumbar
support belts and limit activities, and were placed on light duty
at work. In addition, they were prescribed a nonsteroidal, to be taken
1 hour before therapy and at bedtime during the first 2 weeks of treatment.
After the second week of treatment, medication was decreased and moderate
activity was permitted.
Data was collected
from 219 patients treated during this clinical study. Study demographics
consisted of 79 female and 140 male patients. The patients treated
ranged from 24 to 74 years of age (see Table 1). The average weight
of the females was 146 pounds and the average weight of the men was
195 pounds. According to the Oswestry Pain Scale, patients reported
their symptoms ranging from no pain (0) to severe pain (5).
PATIENT GROUPS
The patients were
further subdivided into six groups:
single lateral
herniation 67 cases
single central herniation 22 cases
single lateral herniation
with disc degeneration 32 cases
single central herniation
with disc degeneration. 24 cases
more than 1 herniation
with disc degeneration 17 cases
more than 1 herniation
without disc degeneration 57 cases
RESULTS
According to the
self-rated Oswestry Pain Scale, treatment was successful in 86% of
the 219 patients included in this study (Table 2, page 39). Treatment
success was defined by a reduction in pain to 0 or 1 on the pain scale.
The perception of pain was none 0 to occasional 1 without any further
need for medication or treatment in 188 patients. These patients reported
complete resolution of pain, lumbar range of motion was normalized,
and there was recovery of any sensory or motor loss. The remaining
31 patients reported significant pain and disability, despite some
improvement in their overall pain and disability score.
Diagnosis MRI
Results on self-rated
Oswestry Pain Scale after treatment.
In this study, only patients diagnosed with herniated and degenerative
discs with at least a 4-week onset were eligible. Each patient’s
diagnosis was confirmed by MRI findings. All selected patients reported
3 to 5 on the pain scale with radiating neuritis into the lower extremities.
By the second week of treatment, 77% of patients had a greater than
50% resolution of low back pain. Subsequent orthopedic examinations
demonstrated that an increase in spinal range of motion directly correlated
with an improvement in straight leg raises and reflex response. Table
2 shows a summary of the subjective findings obtained during this
study by category and total results post treatment. After 90 days,
only five patients (2%) were found to have relapsed from the initial
treatment program.
Percentage of
patients that had improved physical exam findings post treatment.
Ninety-two percent of patients with abnormal physical findings improved
post-treatment. Ninety days later only 3% of these patients had abnormal
findings. Table 3 summarizes the percentage of patients that showed
improvement in physician examination findings testing both motor and
sensory system function after treatment. Gait improved in 96% of the
individuals who started with an abnormal gait, while 96% of those
with sluggish reflexes normalized. Sensory perception improved in
93% of the patients, motor limitation diminished in 86%, 89% had a
normal straight leg raise test who initially tested abnormal, and
90% showed improvement in their spinal range of motion.
SUMMARY
In conclusion,
nonsurgical spinal decompression provides a method for physicians
to properly apply and direct the decompressive force necessary to
effectively treat discogenic disease. With the biotechnological advances
of spinal decompression, symptoms were restored by subjective report
in 86% of patients previously thought to be surgical candidates and
mechanical function was restored in 92% using objective data. Ninety
days after treatment only 2% reported pain and 3% relapsed, by physical
examination exhibiting motor limitations and decreased spinal range
of motion. Our results indicate that in treating 219 patients with
MRI-documented disc herniation and degenerative disc diseases, treatment
was successful as defined by: pain reduction; reduction in use of
pain medications; normalization of range of motion, reflex, and gait;
and recovery of sensory or motor loss. Biotechnological advances of
spinal decompression indeed reveal promising results for the future
of effective management of patients with disc herniation and degenerative
disc diseases. The cost for successful nonsurgical therapy is less
than a tenth of that for surgery. Long-term outcome studies are needed
to determine if nonsurgical treatment prevents later surgery or merely
delays it.
Thomas A. Gionis,
MD, JD, MBA, MHA, FICS, FRCS, is chairman of the American Board of
Healthcare Law and Medicine, Chicago; a diplomate professor of surgery,
American Academy of Neurological and Orthopaedic Surgeons; and a fellow
of the International College of Surgeons and the Royal College of
Surgeons.
Eric Groteke,
DC, CCIC, is a chiropractor and is certified in manipulation under
anesthesia. He is also a chiropractic insurance consultant, a certified
independent chiropractic examiner, and a certified chiropractic insurance
consultant. Groteke maintains chiropractic centers in northeastern
Pennsylvania, in Stroudsburg, Scranton, and Wilkes-Barre.
REFERENCES
Eyerman E. MRI
evidence of mechanical reduction and repair of the torn annulus disc.
International Society of Neuroradiologists; October 1998; Orlando.
Narayan P, Morris IM. A preliminary audit of the management of acute
low back pain in the Kettering District. Br J Rheumatol. 1995;34:693-694.
McDevitt C. Proteoglycans of the intervertebral disc. In: Gosh, P,
ed. The Biology of the Intervertebral Disc. Boca Raton, Fla: CRC Press;
1988:151-170.
Bogduk N, Twomey L. Clinical Anatomy of the Lumbar Spine. New York:
Churchill Livingstone; 1991. Cox JM. Low Back Pain: Mechanism, Diagnosis,
and Treatment. 5th ed. Baltimore: Williams & Wilkins; 1990:69-70,
144. Cyriax JH. Textbook of Orthopaedic Medicine: Diagnosis of Soft
Tissue Lesions. Vol 1. 8th ed. London: Balliere Tindall; 1982. Nachemson
AL. The lumbar spine, an orthopaedic challenge. Spine. 1976;1(1):59-69.
Ramos G, Martin W. Effects of vertebral axial decompression on intradiscal
pressure. J Neurosurgery. 1994;81:350-353. Shealy CN, Leroy P. New
concepts in back pain management: decompression, reduction, and stabilization.
In: Weiner R, ed. Pain Management: A Practical Guide for Clinicians.
Boca Raton, Fla: St Lucie Press; 1998:239-257.
Pal B, Mangion P, Hossain MA, et al. A controlled trial of continuous
lumbar traction in back pain and sciatica. Br J Rheumatol. 1986;25:181-183.
Weber H. Traction therapy in sciatica due to disc prolapse. J Oslo
City Hosp. 1973;23(10):167-176. Yong-Hing K, Kirkaldy-Willis WH. The
pathophysiology of degenerative disease of the lumbar spine. Orthop
Clin North Am. 1983;14:501-503. Matthews J. The effects of spinal
traction. Physiotherapy. 1972;58:64-66.
Goldfish G. Lumbar traction. In: Tollison CD, Kriegel M, eds. Inter-
disciplinary Rehabilitation of Low Back Pain. Baltimore: Williams
& Wilkins; 1989.
Onel D, Tuzlaci M, Sari H, Demir K. Computed tomographic investigation
of the effect of traction on lumbar disc herniations. Spine. 1989;
14(1):82-90.
Back
to top of page